![]()
Original publication date: July 2023
This month, we are honored to feature the Institute for Exceptional Care (IEC), an Rx grant partner who describes themselves as a “do-tank” and stakeholder organization, on a mission to transform healthcare for people with intellectual and developmental disabilities (IDD). In conversation with Dr. Hoangmai (Mai) Pham, President and CEO of IEC, we discuss the liberating framework that is universal design, and how it could transform healthcare settings and practices to ensure that everyone has equitable access to person-centered, high-quality, and affordable healthcare.
Three Things
Human Impact Partners
Watch: A video from Human Impact Partners on Transformative Climate Communities for All: Climate funding for unincorporated communities in CA

The Catalytic Philanthropy Podcast
Listen: Jennie Riley, Rx Foundation’s Executive Director, on a two-part episode

Kaiser Health News
Read: Aneri Pattani’s Meet the People Deciding How to Spend $50 Billion in Opioid Settlement Cash, featuring Rx grant partner Sea Change Recovery Care Organization
Background
Google “targeted universalism,” and up pops a list of links from the Health Equity Resource Library of the Minnesota Department of Health – one of which leads to an animated video that explains the concept in under four minutes.

Developed by Berkeley professor, john a. powell, Targeted Universalism is a policy framework that accounts for the needs of all members of society, but especially marginalized groups. While universal goals are established, a targeted-universalism approach accounts for “how different groups are situated within the structures, culture, and across geographies to obtain the universal goal(s)”.
As health care professionals, advocates, and patients continue to develop strategies to achieve health justice and reduce inequities in healthcare settings, the Minnesota Department of Health and others are exploring how this all-encompassing model might be used to redesign public health strategies so they serve everyone.The Institute for Exceptional Care (IEC), an organization working to transform healthcare for people with intellectual and developmental disabilities (IDD), advocates for universal design, a concept similar to targeted universalism that recognizes everyone has different needs.
IEC was founded in 2020 by healthcare experts who know the anxiety of seeking services for loved ones with disabilities. Through all of its programs, IEC centers the perspectives of people with disabilities. Self-advocates participate in every project and serve in leadership roles on IEC’s Board. By bringing together the IDD community and healthcare leaders, IEC facilitates collaborative problem-solving and promotes sustainable change at scale through programs including the Action to Build Clinical Confidence and Culture and the Seamless Care Alliance of Nassau and Suffolk.
Last May (‘23), Dr. Mai Pham, founder and leader of IEC, and the mother of an autistic young adult, joined the Rx Foundation for a Power is a Social Determinant of Health session titled, “Making Disability a Priority in Health Equity: How Do We Accelerate Change?”. Dr. Pham shared discoveries from IEC’s work, including lessons on authentic engagement, universal design, and advocacy.
During her presentation, Dr. Pham explained why, in her view, such a liberating model – a framework that acknowledges and normalizes that everyone has different needs, removing unnecessary barriers and leaving room for more autonomy – has not been systematically implemented in healthcare settings.
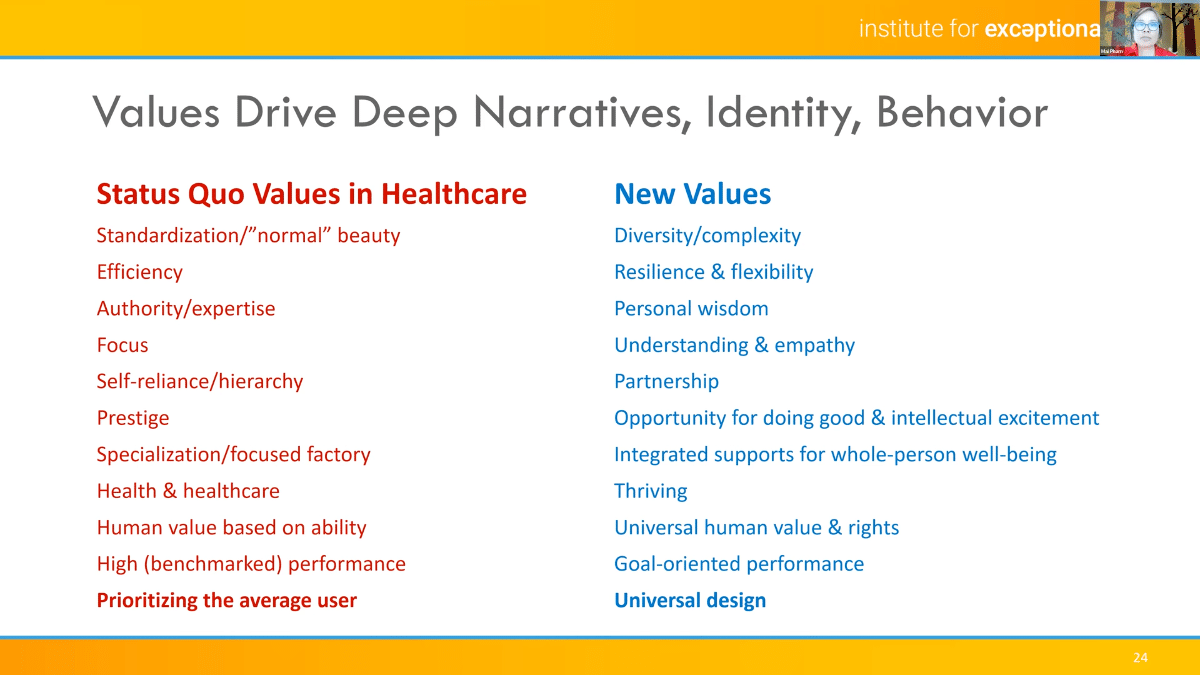
In healthcare, there is a set of unspoken status quo values that drive behavior and practice. In the slide shown below, you can see the tension between competing values such as “efficiency” and “resilience & flexibility”. However, a universal design approach holds space for both of these seemingly competing values. Dr. Pham gave the example of a physician who prioritizes, by training, efficiency in clinical visits with patients. But if a physician can be a bit more flexible and resilient with patients, over time, the provider will actually become more efficient because flexibility and resilience – rather than a strict, unyielding adherence to efficiency – will result in fewer mistakes and costs incurred.
Concern about the drawbacks of thinking in binaries in healthcare is not new, as others have noted, but the problem persists. IEC is a compelling case study in how organizations can embrace and apply a both-and strategy, breaking bifurcation in service of a universal health justice goal, or in the case of IEC, making disability a priority in health equity.
In our conversation below, Dr. Pham expands upon these core lessons from the perspective of being both a healthcare insider “do-tank” and a stakeholder organization, representing both healthcare professionals and IDD change agents. While she offers insights specifically related to IEC’s advocacy alongside people with IDD, she shares broad lessons applicable to any organization advocating for individuals, families, and communities that are not adequately served by – and, in many cases harmed by – the status quo.
In Conversation with Dr. Mai Pham
(Cook, Rx): Can you explain what universal design is and how it could transform how we all receive healthcare, including people with IDD?
(Pham, IEC): Universal design is the concept of designing anything – whether that’s a tool, a process, or a physical environment – so it can be used easily by as many people as possible.
Universal design does a lot of things. First, it heightens our awareness. It broadens our understanding of what is “normal”. It allows for diversity but normalizes all the outliers. Not only does it send that signal but it also trains the clinical brain to then look for outliers. That curiosity can take you a long way if you listen to it because you will then inquire about things that may not be visible to you.
Universal design doesn’t leave people behind. Even if one is privileged enough to be really independent and resilient and adaptable at the best of times, none of us lives there our whole life. Universal design creates a safety net for when people are either born needing more supports, or when people develop new problems somehow and need more supports for a stretch of time in their lives.
One thing that I’m appreciating more and more, is that universal design, when implemented, actually frees up a ton of time and energy, including mental work and resources for us to address other problems. Knowing that there will be accessible elevator doors and bathrooms, and curb cutouts around the hospital means I don’t have to worry about those things anymore if I need them, or for a kid on crutches. I can focus on other things. Similarly, if health education materials are in plain language with pictures and there’s a button that you can click to hear it verbally, in plain language, I’m good to go. From the provider perspective too, I need to stress less about having to mimic that in my precious clinical time with a patient.
Universal design is liberation for everyone. I use the word ‘serve’ a lot when I talk about what clinicians need to do with patients with IDD because I think it’s a word that everyone understands and it’s short, but really what I think happens when the healthcare team engages in this kind of work is that they too are liberated. It’s co-liberation. I don’t think many of us believe that most clinicians feel “free” in today’s system. There’s something nourishing and freeing and empowering for all involved with universal design. You have solved common problems that allow you then to go on to more important, trickier problems. And you have eased the burden on everyone. And I think that maps the real potential of it.

(Cook, Rx): How do we redesign our healthcare system to scale so that everybody can receive universally designed, person-centered, high-quality, and affordable health care when they go to their hospital, primary care provider, and other clinicians?
(Pham, IEC): It depends on the sector you’re talking about. Thinking tactically and strategically – the insurance sector has so many legacy barriers. There are legacy data systems, fragmentation problems from the employer-based insurance model, and professional standards – all of which get in the way. In a sector like that, I think about finding an initial handful of adventuresome partners to try something new with the promise that it will differentiate them in the marketplace. And it catches fire. For example, what if one insurer created a truly user-friendly, plain language version of their “open enrollment” process when a person has to choose their health plan each year? The ways it can catch fire is some big employer adopts it and runs with it and other big employers hear about it and become envious.
In a clinical setting, I’d go at it in a much more wholesale way by including concepts of universal design as part of the training package in our ABC3: Action to Build Clinical Confidence and Culture Initiative, which is scaling strategies to engage, prepare, and support general clinicians in providing better IDD care. And when we’re ready, going out to professional societies and saying “Not only is there learning about clinical care people with IDD, but also [there is] an opportunity to do practice redesign that will make help all your patients”.
The hardest sectors to get to move will be the ones that will need to change bricks and mortar and legacy technology.
(Cook, Rx): What has held us back from systematically implementing universal design?
(Pham, IEC): I think the real culprit behind not driving universal design is this worship that we have of the “average patient” or the “median” patient. It is how hospital quality leaders, patient experience officers, data scientists, health care researchers, and government officials walk around thinking. They know there are outliers, and they are always concerned about those, but it’s not who the system is designed for. That’s the problem. The perversity of it is that when you do that, you end up serving maybe one person well: that unicorn person who manages to stay in the median their entire lives. Everybody else moves around on the bell curve. You don’t get to dictate where anybody is on a given day.

Somebody recently asked me after a presentation, what does “universal human value” mean?
When IEC first got started, we had so many exploratory conversations like “Hi! Who are you? Here’s who we are! Here’s what we think we want to do, what do you think?” I mean hundreds of those conversations. And we would take notes. But we didn’t have a customer-relationship system at the time so they all went into one Word document, serially. We called that document the “Small Treasures” doc.
The reason we called it that was because when my autistic son Alexander was little, whenever he went outside, he would pick things up. He was the smallest in the family – now he is the tallest, which is very funny – but that meant back then, he was closer to the ground. So that’s what we assumed it was, that he was better able to see interesting things down there. It took us a while to notice that whenever he came back from being outside his fists would be closed. We only noticed when we needed him to do something with his hands and he couldn’t because his fists were closed. We’d pry them open and inside would be small things that he had found. It might be the tiniest bit of perfect purple glass or a sliver of mica, or the perfect fern frond, just some real unusual curiosity. And I learned to put them on a shelf. I would just let them sit there until I sensed they had lost their magic for him, and then I would get rid of them. This is how, for example, we ended up with sand art tubes for eight years, or why we still have so many darn fossil rocks – that’s how long it took for them to lose their magic for him (laughter). But I remember once saying to him, “Alexander, you find the best treasures” and he looked at me and said, “You are the only person who understands that.” And I told him right back, “It would be an honor to see the world the way you see it.” I realized that he was teaching me. He became my meditation strategy. He became my go-to for not just slowing down, but seeing and being mindful. He was teaching me quite explicitly how to see beauty and value in things that other people considered trash. He carries that throughout the way he lives his life – I still find things on his windowsill.
We went to a family summer dance and music camp every year since my sons were little, and when Alexander was six or seven, the staff person leading the littles that year had them make little illustrated bookmarks with some inspiration from nature. Alexander’s contribution was “Queen Anne’s Lace is nature’s fireworks, and the pollen is its smoke”.
That’s universal human value.
(Cook, Rx): What is your North Star, or what brings you hope?
(Pham, IEC): The hope part is easy – what brings me hope is people like that guy (Pham points the webcam to her son in the kitchen). That’s Benjamin, Alexander’s older brother. I think younger generations give me a lot of hope. They’ve grown up in a much more diverse and difference-aware world and they’re fine with it. It’s like breathing air to them. And that gives me a lot of hope, young people.
What’s my true North? It’s a little complicated. In Judaism there’s this term tikkun olam, and it means healing the world. The short version of the answer is that when we, at IEC, can bring together people with disabilities and really powerful healthcare decision makers, and create this space for them to not just work together but see each other and do a little bit of that rebuilding of trust that to me feels like setting a table for people to gather together to break bread. That is tikkun olam.
More from the Institute for Exceptional Care

Power is a Social Determinant of Health: Institute for Exceptional Care
In this recorded webinar, hosted by the Rx Foundation in June 2023, Dr. Mai Pham, founder and leader of Institute for Exceptional Care (IEC) and mother of an autistic young man, shares how IEC is working to make healthcare better and safer for people with intellectual and/or developmental disabilities (IDD) so they and their families can lead their best lives.
IEC has made some surprising discoveries about “authentic engagement,” what makes for effective change agents, and the unique opportunities for IEC to drive change as it straddles being both a healthcare insider “do-tank” and a stakeholder organization. These discoveries are informing IEC’s launch of an IDD Advocate Corps that will bring together professionals within healthcare who want to drive change in their own organizations to improve care for people with disabilities. Pham engages the group in discussion about how this model and new kinds of partnerships could be applied to other areas of advocacy for individuals, families, and communities that are not adequately served or even harmed by the status quo.

Connect With Us on Social Media
Follow-us on social media for the most up-to-date news, resources, and events from the Rx Foundation and its partners.