![]()
Original publication date: June 2023
This month, we are honored to feature the Health and Reentry Project, an Rx grant partner whose mission is to “improve the lives, health, and safety of people and communities…by building bridges across sectors and stakeholders, advancing policies that promote continuity across carceral and community healthcare settings, and accelerating and scaling innovative approaches to reentry health care”. In conversation with Vikki Wachino, Founder of HARP, and Margot Cronin-Furman, Chief of Staff, we discuss Medicaid’s new groundbreaking policy guidance that offers states the ability to cover health services for people leaving carceral settings and returning to their communities – and the broad impact the policy will have on all people affected by incarceration.
Three Things

Leveraging the Healthcare Sector to Deploy $80B in Unused Federal Aid
Watch: A webinar from Dr. Alister Martin, CEO and Founder of A Healthier Democracy
Leveraging the strengths of public health & health care for a healthy democracy
Listen: Aliya Bhatia (Executive Director of Vot-ER) and Jeanne Ayers (Executive Director of Healthy Democracy Healthy People) on County Health Rankings & Roadmaps’ In Solidarity podcast
In California’s Heartland, a New Resistance Movement Is Taking Root
Read: Mark Arax for the New York Times
Background
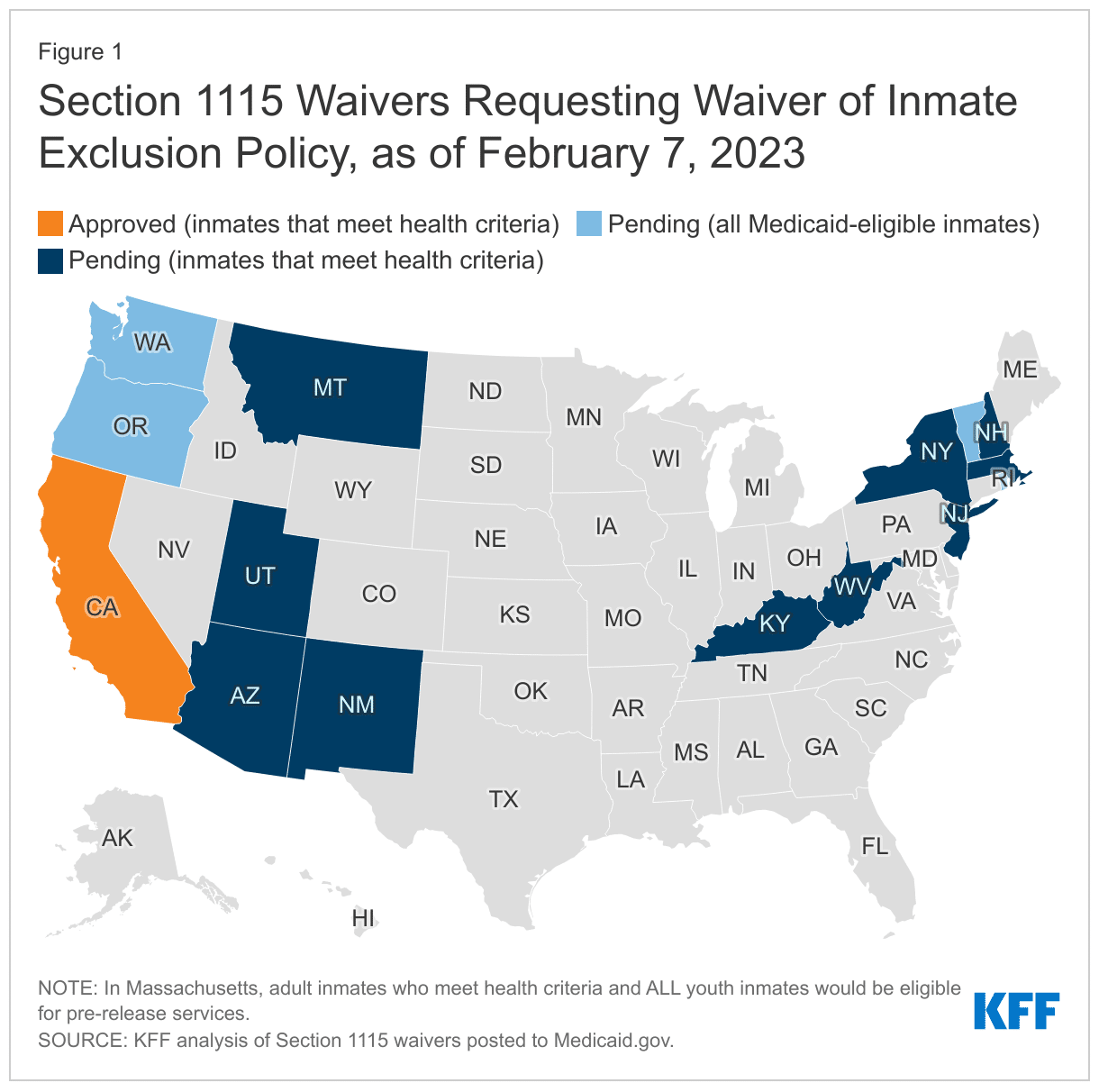
In April 2023, Health and Human Services (HHS), through the Centers for Medicare and Medicaid Services (CMS), announced groundbreaking new policy guidance encouraging states to strengthen health care access at the point of reentry to improve people’s health and wellbeing as they return to our communities after incarceration.
The Medicaid Reentry Section 1115 Demonstration Opportunity waiver guidance offers state Medicaid programs the ability to cover health services for people leaving carceral settings and returning to communities, with a goal of improving access to healthcare services and continuity of care.
This is the first time that Medicaid will cover pre-release services while people are incarcerated, and those services may be covered for up to 90 days prior to release.
The policy was informed directly by input from health and justice leaders and advocates, including the Health and Reentry Project, formed in 2022 as a collaboration among the Council on Criminal Justice, former CMS Deputy Administrator Vikki Wachino, and Waxman Strategies. The goal of the Health and Reentry Project (HARP) is to advance policy and practice to improve lives, health, and safety as people return to communities after incarceration.
That CMS issued this waiver guidance on Medicaid coverage prior to reentry is a monumental win, first and foremost, for the individuals and communities directly impacted by incarceration.
At this moment, as Vikki Wachino described, “we are starting to re-examine Medicaid’s role and for the first time ask ‘How can we meet people’s health needs as they are leaving prison and jail? Can we start connecting with people before they leave, with Medicaid’s support, to provide a set of services such as case management and medication assisted treatment for people who need it – and by doing so blaze a path to having their needs met in the community?’ We are essentially building a bridge and connection points to the outside, linking not just health but potentially also housing, nutrition services and other supports to help people get back on their feet, reunite with their families, and rejoin our communities successfully.”
Historically, the health and criminal justice systems have generally been strangers to each other. As Vikki Wachino explained, “There are very few touchpoints between the community health care system, which those of us who are not incarcerated experience, and the correctional healthcare system. When people are in prison or jail, there is very little transparency around the healthcare services that they receive. The infrastructure that those of us who visit health care providers in the community are accustomed to – electronic health care records, benefits and claims, etc. – they only exist in carceral settings to a limited extent. But what makes this a potentially high-impact moment is we’re recognizing that these two highly siloed systems need to recognize each other, and that’s where these new policy changes around Medicaid really come in. This has the potential to be a transformative moment.”
In our conversation with Vikki Wachino and Margot Cronin-Furman below, we learn more about the groundbreaking new policy and its potential impact for formerly incarcerated people and communities affected by mass incarceration. They share more about HARP’s policy recommendations, how Medicaid coverage at the point of reentry can improve health outcomes, and the ways in which health systems and providers can get involved.
In Conversation with the Health and Reentry Project (HARP)
(Cook, Rx): When reading the policy recommendations released by HARP, I was struck by the Navigator model, which is similar to the Community Health Worker model. Can you speak more about this idea of a Navigator model and how critical that component is for improving health outcomes for justice-involved people at the point of reentry? What about that model is particularly effective at connecting these siloed institutions, benefits and services that they could have access to?
(Wachino, HARP): This recommendation, like all of the recommendations, came directly from the feedback of over 70 stakeholders who engaged with HARP. When we asked them, “what do we really need to do to make this system work for people?”, the idea of having a patient-navigator model was essential.
We need to build greater trust in the healthcare system. Many people who are in prison or jail have not interacted with the healthcare system for some time before coming to prison or jail. And there’s also mistrust. People coming out of prison or jail need some assistance in navigating these very complex systems at a time in which they have a lot of other things going on in their lives too. They are scrambling for housing and food, to find their family members and reconnect with them if they have been disconnected.
The idea of a Navigator is to have someone, who has lived experience with the criminal justice system, support people returning to their communities. One notable model of this has been the Transitions Clinic that started in California. It is a primary care-based health center model that includes community health workers with lived experience. We have an opportunity to train a cadre of people including people who themselves have experienced incarceration, to help people navigate systems
The last point I’ll make is around people with lived experience being involved in policy development and implementation. This is critical. Very few of us on the outside have an idea what it is like to be on the inside. I, for all of my years of healthcare experience, cannot guess. I shouldn’t guess as to what those conditions are like or as to what is actually going to meet people’s needs. People who actually experienced it need to be invited to the table and placed in roles, including but not limited to community health workers or Navigators, to actually lead and assist in both the development and service delivery pieces. That has been one of the most important learnings for me from our work so far through the HARP – the value of having people directly at the table who I can learn from about what it is that they’ve experienced and what they needed as they were returning to their communities.
(Cronin-Furman, HARP): I think about the reentry Navigators in the context of what I’ve seen in other healthcare settings. For example: many oncology practices have patient navigators available to support patients because they acknowledge that a cancer diagnosis is a life-changing moment. Similarly, reentry is a life-changing moment. And you need somebody who has been there before, who knows what the resources are and can walk the path with you. There is something so powerful about making sure that people are not alone and have somebody that they can trust to support them as they navigate the transition
(Cook, Rx): What lessons have you learned from building a coalition of stakeholders, where folks may hold conflicting perspectives about the criminal justice system. How did you build consensus?
(Wachino, HARP): It’s really interesting because when we created HARP, we committed to bringing cross-system actors together: people who have worked in prisons and jails, community corrections, law enforcement courts, health care providers, Medicaid officials, community leaders, advocates, and as we’ve already discussed, people with lived experience. This is rarely done, but is essential to improving health and safety – and to making these new policies work. You might not expect these diverse stakeholders to have a lot in common. But we quickly saw a broad consensus emerge. We didn’t see universal consensus. Of course, you never do. Perhaps that’s not the right standard though. It felt important to bring everyone around the table to talk and, importantly, listen. When we did that, what was remarkable was the high degree of alignment that we heard about what was needed across a variety of stakeholders. I think if we back away from the binary of “this is good” or “this is bad” and ask, “what is it that people need to succeed?” I actually don’t think there’s a lot of debate about that. It’s pretty clear what people need to succeed at reentry – a supportive bridge, patient navigation, someone to listen and help them get back on their feet. We did not hear much disagreement about that.
(Cook, Rx): That’s remarkable. And I think that goes back to health being a particular lever or entry point for these larger conversations. It’s interesting to think about ways we can open doors to other topics through the lens of health because it cuts across so many interlocking elements, like racial justice and criminal justice, among others, in this case.
(Wachino, HARP): That’s right. Health is essential. If you have your health, you have so much. It’s foundational to your ability to enjoy your family, to work, to participate actively in your community – and it promotes community safety. It’s foundational to everything else.
I think during the conversation we’ve talked a lot about the people who are incarcerated themselves but if you take a step back from that and we think about the effect incarceration has on families or communities, it’s not just the nine or ten million people who go in or out of jails every year. It’s their community they return to, their family members, too. Families who are affected by incarceration are deeply impacted by incarceration. They lose their family member for a period of time – that could be days, weeks, months or even years – that’s a huge absence for them. It very much affects people’s ability to parent, to form relationships with their children. And it affects communities too. If you are living in a community that has a lot of people who have been adversely impacted by incarceration, or who haven’t had their healthcare needs met appropriately, it’s going to have an impact on the health of the entire community.

Medicaid has the potential to connect eligible people leaving jails and prisons to services that can maintain or improve their health and mental health, financial security, and ability to participate fully in their families, their communities, and the workforce.
– HARP’s “Redesigning Reentry: How Medicaid Can Improve Health and Safety by Smoothing Transitions from Incarceration to Community”
One wish I have for this work is to see it not just as affecting the group of people who have been incarcerated themselves, but also how it affects larger ecosystems, communities, and families. And needless to say, it affects the outcomes that we get from our criminal justice system. The impact of reentry is extremely large and affects a whole variety of people that reside in concentric circles around the person who has actually been incarcerated themselves.
This is a moment for action. And that’s unique. We have a new policy groundwork laid; and it’s groundbreaking. We, as people who work in the healthcare system, need to figure out how we are going to make this work and make the most of this moment. And, crucially, health leaders need to work with public safety leaders. This is not just a big change for health care. This is a big change for criminal justice. This is an opportunity to deliver on public health fundamentally. And I hope that all of the different people and organizations and stakeholders that care about public health, and those that care about public safety, really rally around this and collaborate to make it work. And the “making it work” will be challenging. We need to be thoughtful and committed about implementation, which will make some big asks of both correctional and health care leaders. There is high-impact potential, but we need to all be ready to roll up our sleeves and get to work.
(Cook, Rx): How can folks working in the healthcare setting get involved in this work?
(Wachino, HARP): I would say, first, take a moment to learn about the criminal justice system and who it is affecting and how. And, get to know the public safety actors in your community – sheriffs, departments of corrections, local jails, courts, probation and parole. Some of them are struggling to meet peoples’ health and mental health needs and looking for ways to do it better. Then think about the specific ways in which all of the different actors and organizations in the healthcare system can be meeting those needs. Community health centers have a vital role to play here. Managed care organizations have a vital role to play here. All kinds of providers, including mental health providers. I don’t think there’s one way to get involved, it’s more “how do we mobilize the different type of organizations that can really deliver here?” and “how do we help them to understand the needs of this specific population?” and “how can we understand the perspective of correctional entities, whose active involvement and commitment to change is needed to make this work?” We all have a lot to learn there. And can we redesign service delivery to meet those needs? And, critically, changing service delivery is not just about reentry services. It is about making sure that people have access to community health and behavioral health services at all points in their lives, and the potential for that increased access to help people avoid the correctional system in the first place.
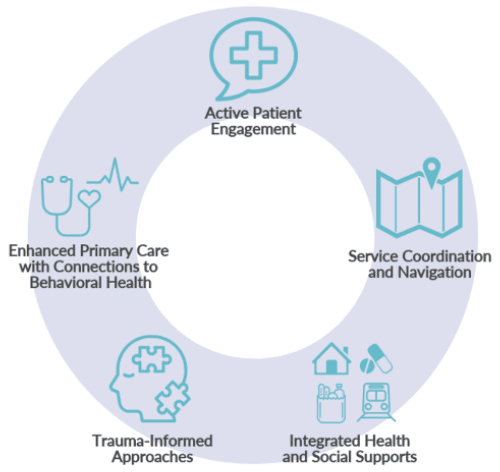
I think the thing that most strikes me about the first phase of our work is that, with cross-sector stakeholder feedback, we developed a reentry care model. The care model says – as people are released, connect them to primary care and behavioral health services, and add in social support services, patient navigation, and trauma-informed care. I now have people calling me saying “I’m talking to this managed care organization, who wants to do this work. What should I do?” My answer to that is look at the care model and find ways to deliver and pay for services that advance this new standard of care that we think has the potential to deliver for people as they return to their communities.
(Cronin-Furman, HARP): This isn’t an issue that just affects people who are justice-involved. Every provider should look at their patient list and ask, “am I taking care of people who are affected by incarceration?” Because even if they think they aren’t, they absolutely are. Their patients might not have direct experience of incarceration but may be friends or family members of people who are or have been justice involved. The widespread impact of incarceration on health means that this cannot be just the work of organizations that are focused on taking care of people who are coming out of the criminal justice system. It needs to be a universally held belief that people who are affected by incarceration deserve care and respect, no matter the setting.
(Wachino, HARP): Yes, and how do you provide an environment where someone is comfortable sharing their justice-involved status or that they’ve been affected by incarceration? One thing that struck me since I’ve started doing this work is the number of people who I’ve known for some time, who have told me for the first time that they had a family member who was incarcerated. We have to create an environment where people are open to talk about it.
The other interesting thing on the provider front is that sometimes the provider experience of providing care to incarcerated people is that they have a patient, they have a relationship with the patient, and, from the provider perspective, the patient just disappears for some period of time. Who knows how long that time period is, and then suddenly they come back. And the provider wonders, where have you been? They do not know that the patient has been in prison or jails. And tries to meet their health needs. But they can’t make up for that gap in time. What these new policies create is some degree of continuity so it feels like less of a gap to the provider too. They are getting some information about the patient and where they’ve been. And then of course the provider has to be very open to the patient and their needs. As healthcare providers, as clinicians, people should be motivated by the ability and interest in providing the clinical services people need and put judgment aside and create an environment where there are patients who are open to discussing the circumstances of their lives.
(Cook, Rx): For our final question, what is your North Star?
(Wachino, HARP): I think throughout my career, I’ve been most motivated by the idea of helping the people who have the most needs. That’s what brought me to Medicaid in the first place. As I’ve gone on in my career, I’ve found that there’s additional value in looking not just at the needs of people who are poor but at specific populations too. I think my North Star is trying to find a way to make the healthcare system work for the people who most need it.
(Cronin-Furman, HARP): My background is as a healthcare social worker, and what I used to say to trainees is that you need to be competent and kind. If we can build systems that treat everyone, no matter how stigmatized their identity or complex their needs, with competent care and do it with kindness and a trauma-informed perspective, then we’re moving in the right direction.
Resources from the Health and Reentry Project
Breaking Ground: How California is Using Medicaid to Improve the Health of People Leaving Incarceration
California was the first state to receive federal approval to cover select services through Medicaid in the period before a person leaves prison, jail, or a youth correctional facility.
In a recent report, Margot Cronin-Furman, Vikki Wachino, John Sawyer, and Silicia Lomax detail California’s latest reforms at the point of reentry, authorized under the Medicaid Section 1115 demonstration waiver, including their projected impact and implications for both those directly affected by incarceration and other states considering similar reforms.
By using California as a case study, the report offers health and criminal justice policymakers at both the state and federal levels a roadmap and series of recommendations related to their own efforts to achieve a continuity of care and other services at the point of reentry.

Medicaid and Reentry: New Policy Advances Webinar
In April 2023, the Centers for Medicare and Medicaid Services issued new national guidance to states on how to provide Medicaid covered services at reentry through demonstration waivers. The guidance builds on the federal approval in January of California’s plan to cover some services for 90 days pre-release, a first-of-its kind policy change. This change carries enormous potential for public health and public safety: successful implementation of these policies can drive health goals and justice reform goals alike by facilitating continuity of care, access to needed treatment, and connections to community-based services and care providers.
On April 27th, the Health and Reentry Project’s Executive Director Vikki Wachino moderated a webinar featuring two of the leading federal officials who developed this landmark new reentry policy – as well as from health and justice leaders working to translate the promise of policy into meaningful changes for people’s lives in communities.

Connect With Us on Social Media
Follow-us on social media for the most up-to-date news, resources, and events from the Rx Foundation and its partners.