![]()
Original publication date: February 2024
This month, we are honored to spotlight Dr. Roseanna Means and the Bridges to Moms program at the Brigham and Women’s Hospital. We first connected with Dr. Means in 2017, but recently reconnected to chat about what pregnancy care looked like for women experiencing homelessness in Boston prior to BTM, her lessons learned from eight years of programming, and what systemic changes are still needed to make birth equity a reality for all. It’s a remarkable story that underscores the importance of addressing social drivers of health, and offers a roadmap for other direct services providers, no matter the focus area or initiative.

Engaging Community Organizations in Redesigning Reentry
Watch: A Power is a Social Determinant of Health webinar with the Health and Reentry Project (HARP)
Turn on the Lights Podcast
Listen: Episode on “Investing in Local Communities to Improve Health”

Nonprofit Quarterly
Read: “Hope Is a Practice and a Discipline: Building a Path to a Counterculture of Care”, an excerpt of Kelly Hayes and Mariame Kaba’s book, Let This Radicalize You: Organizing and the Revolution of Reciprocal Care
Background
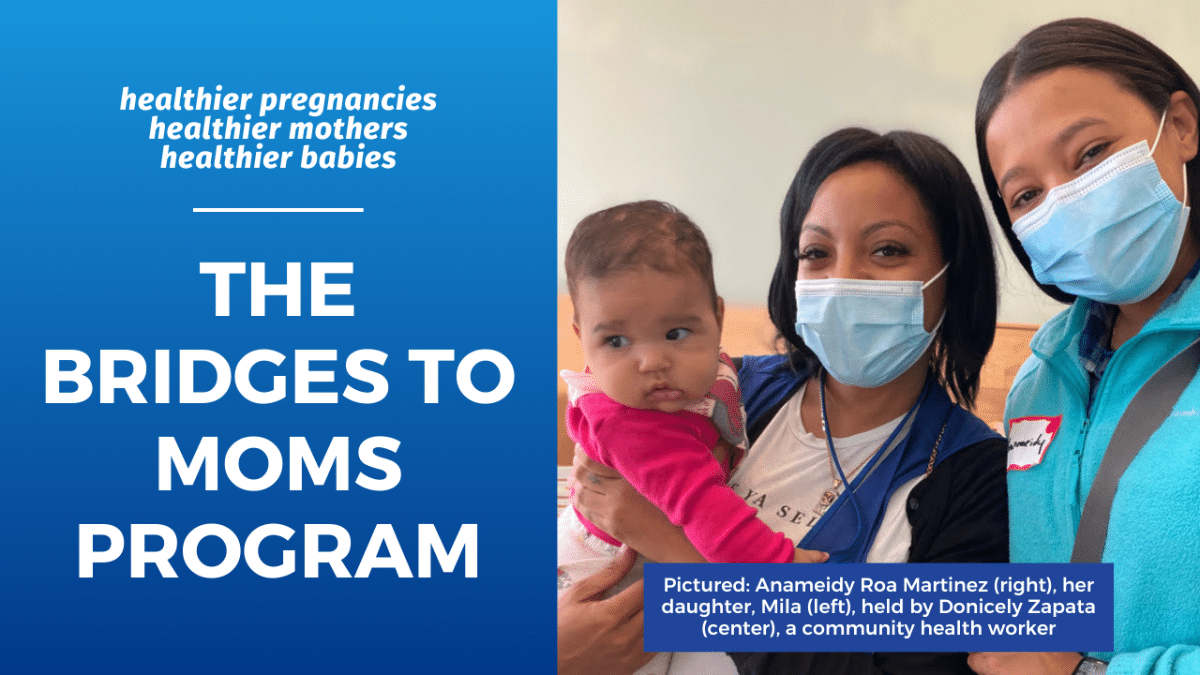
When Anameidy Roa Martinez, 29, first connected with Bridges to Moms, she was pregnant, unemployed, and on the cusp of losing her housing.
At around seven months of pregnancy, she suddenly experienced such severe pelvic pain that she had to leave her job as a daycare teacher. “I couldn’t walk, run or pick up the kids. I couldn’t do anything. It was painful to even take a walk outside,” she recalled.
Living alone, Ms. Martinez quickly fell more and more behind on rent; and as she approached her due date, losing her housing was becoming more and more possible.
“It’s the first time I’m dealing with something like this — not knowing how I’m going to pay the next month, what’s going to happen with the amount that I owe now, if I can get a job,” she said. “I have to have a roof over my head not only for myself but also my daughter. That’s the most stressful thing I’ve been going through.”
When she mentioned her housing situation to a social worker during one of her prenatal visits at the Brigham and Women’s Hospital, Ms. Martinez was immediately referred to Bridges to Moms.
Ms. Martinez’s story is just one of hundreds of women, a majority who are women of color (90%), who have faced unimaginable challenges during their pregnancy and motherhood, including not knowing where they can take their newborn home to following delivery, but were eventually connected to Bridges to Moms.
In 2016, Bridges to Moms (BTM) was founded by Dr. Roseanna Means, attending physician in the Division of Women’s Health. BTM is a philanthropically supported program at the Brigham and Women’s Hospital that aims to bridge the multiple gaps in health care and social needs for pregnant women facing homelessness or housing insecurity.
Since inception, BTM has assisted over 600 women facing homelessness or housing insecurity, poverty, and domestic violence, and so forth. Women, like Ms. Martinez, are welcomed to the program and provided with housing supportive services, transportation, food, and various community resources by an expert team of bilingual community health workers, housing specialists, and case managers. Welcome packets also include tangibles for basic health-related needs, including tickets to the Brigham’s cafeteria, Stop & Shop and Target gift cards, and more. BTM provides and pays for all transportation to prenatal and postpartum medical appointments, sometimes as far as 50-70 miles from a shelter to the hospital, in order to ensure healthy birth outcomes. BTM also pays for moms to be transported to their babies in the NICU for every day of the babies’ hospitalizations so that the moms and babies can bond. The BTM team works side-by-side with the women in an outpatient setting, throughout their pregnancies and during the baby’s first year. Their primary health equity goals are to improve prenatal clinic attendance, gestational age at birth, birth outcomes, and maternal bonding, and reduce NICU stays; BTM achieves these by attending to the social drivers of health.
Their approach has proven immensely successful. The moms enrolled attend nearly all of their prenatal visits; over 90% successfully connect with a primary care provider postpartum; and no BTM mothers have died. These results mean healthier pregnancies, stronger maternal bonding, and healthier outcomes for mothers and their babies.
During a woman’s postpartum year, the BTM team also helps people move forward in their health and self-sufficiency by connecting them to ongoing primary and mental health care, and steering them to Workforce Development Training programs, GED classes and ESL classes. Most recently, last October, BTM hosted its third annual Career Day. Over 70 moms and babies visited the Brigham’s Hale Atrium for a day full of skill-building in resumes, finance, budgets, and interviewing.
The Rx Foundation first connected with Dr. Means in 2017, when we made a grant to strengthen the staffing capacity of BTM, and ultimately expand the number of women served by this innovative case management model. We recently reconnected with Dr. Means to chat about what pregnancy care looked like prior to BTM, her lessons learned from eight years of programming, and what systemic changes are still needed to make birth equity a reality for all, including those facing homelessness.
(Rx): Before Bridges to Moms, what was the experience of a pregnant person experiencing homelessness in Boston? Can you walk us through what pregnancy care, delivery, postpartum care looked like? And how things changed for women through the pilot?
(Dr. Means): In 2015, I was approached by the Head of Care Coordination at Brigham and Women’s Hospital, where I’ve been on staff as a physician since 1981. They were inquiring about the problem of women experiencing homelessness who were pregnant and coming to the hospital for maternity care – what would happen when they were discharged with their newborns? Where would they go?
I had extensive experience working with homeless people at the Brigham, through the Boston Health Care for the Homeless program, where I worked from 1990 to 1998, and my own nonprofit, Health Care Without Walls, which I had run since 1999. I knew from my experience as an expert in women’s health, and as somebody who had worked in the field of homelessness, that what happens outside the walls of the hospital when you’re discharged is pretty much invisible to the healthcare system – how people get there, how people get food, whether it’s enough food, all kind of factors.
The Brigham and Women’s hospital accepts high-risk pregnancy patients. So pregnant people experiencing homelessness would be referred to the Brigham, often with limited health insurance, covering only prenatal care and a couple of postpartum visits. Under coverage, they would receive four or five days in the hospital if it was a cesarean birth, or one to two days if it was a vaginal birth. And all women would be discharged the way we all did when we had our children – they put you in a wheelchair, they take you down to the front door with your baby in your arms and then they let you go into the wild world.
People like me have somebody who picks us up in a car and we’ve already bought a car seat; we get the baby strapped in and we go home. Our neighbors have dropped off casseroles, or a mother-in-law is waiting at home to meet their first grandchild. People have had a baby shower and received a stroller, baby blankets and spit-up cloths – everything you could possibly want for your baby. But women who are experiencing homelessness would get to the front entrance of the hospital, and that’s where the hospital is kind of done with their part of it. In most cases, these women would call a cab and go down to the state housing office, then called the Department of Housing and Community Development (DHCD) (now Executive Office of Housing and Livable Communities, or EOHLC for short).
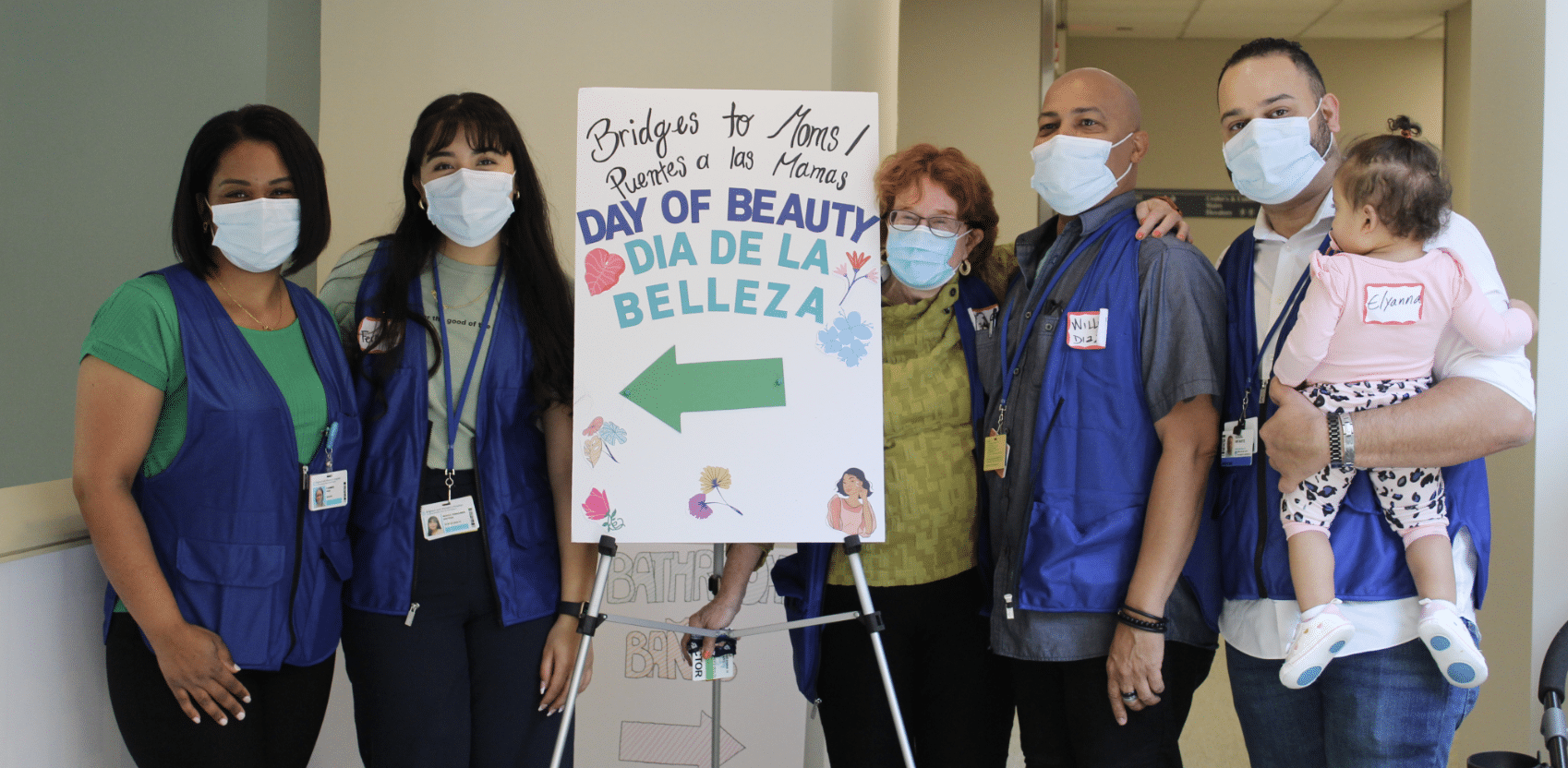
Members of the Bridges to Mom team, from left: Carmen Peña, Fernanda Ortega, Roseanna Means, William Diaz and Edual Infante (with his daughter, Elianna).
PC: Brigham and Women’s Hospital
EOHLC is first-come-first-served. When hospital discharges took place in the afternoon, as most do, these women would arrive at EOHLC when all shelter beds were already allocated. Women would sit there with their newborn, as young as two days old, looking for a place for the night; and a case manager would often say, “I’m sorry, there’s no more places for tonight”. So, these recently postpartum women would be left calling someone they barely know, or a friend, or even the baby’s father or mother-in-law, who she might not be speaking to because it’s an unsafe domestic situation. She would try to spend the night wherever she could and come back the next day and do the process all over again. It was really uncertain and scary for the moms. They had nothing, they had no stuff for the baby, no place to take the baby, no food for the baby.
So when the Care Coordination person at the Brigham said, “can you please help us come up with a way to help these patients knowing what you know about homelessness?”, the first thing I did was learn what was going on, what the reality was. I spoke to the social workers. There were a lot of tears. A lot of people said, “this is so frustrating. I go home at night and I’m worried about these families, what’s happened to them, what’s going to happen to that baby”. People really felt powerless because they had no information about what was going on.
I decided to look at it through the lens of the social determinants of health – how does the mom get here? What does she have for support? What is her primary language? Who can she call in the case of an emergency? Does she have any resources whatsoever? Does she have any food, and is it the right kind of food? Does she have medical conditions that require her to have a certain diet? Is she eligible for food stamps? Was she even getting WIC? So, I looked at every little step, and to a very granular level. I figured out the priorities. Housing and food were huge, transportation too. If the women can’t get to their prenatal and postpartum care, it not only puts their pregnancy at-risk but also their personal safety.
I created a pilot program for the hospital to manage these patients, first by hiring staff from the nonprofit I ran, Health Care Without Walls, to fill in the coordination gaps for housing, food, transportation, safety, and so forth. We hired a field team of community health workers and nurse practitioners, and we collectively came up with a community outreach program where we could address all of these things for the women who came to the Brigham. So these women, who were once discharged from the hospital with nothing and getting in a cab to locate a shelter for the night, were now connected with a compendium of services that we offered in the pilot. We connect them to food stamps, housing, and transportation. We referred them to programs that would put them in a safe place.
It ran for two years, and what we showed was that women were actually attending a majority (>90%) of their prenatal and postpartum appointments because we were providing the transportation to get them there. They were being housed safely. There were no maternal deaths. In all, there was actually quite an impact if you did provide this personalized care. It was really what every woman needs to get through a difficult pregnancy without resources. At the end of 2021, when I retired from Health Care Without Walls, I moved the whole program in-house at the BWH. Now Bridges to Moms is thriving at the BWH and we are able to accept more referrals and build more collaborations.
(Rx): I think what really stuck out to me is remarkably, you have had no maternal deaths since operating the program. The population you’re serving is mostly women of color, who are experiencing maternal mortality rates five times higher than white women, in addition to being homeless. What do you attribute to that success? What lessons do you have about that?
(Dr. Means): It’s a figure that I’m really proud of because we’ve now helped over 600 women. We’re going through our eighth year. Ninety-five percent of people we serve are women of color, and not a single maternal death.
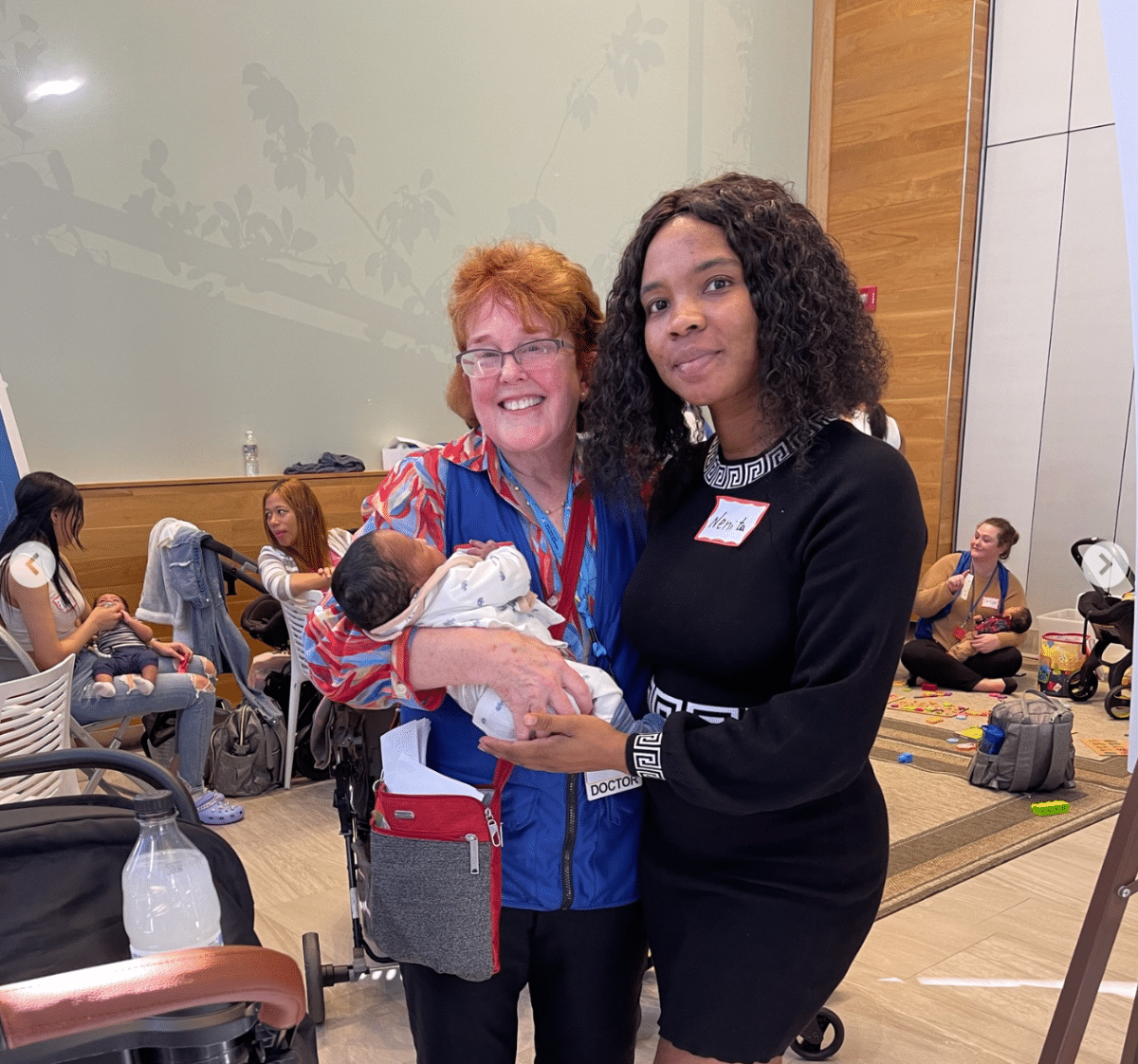
Baby S., pictured being held by Dr. Means, is a Brigham NICU graduate and enrolled in the Brigham Transition to Home Program!
PC: Brigham and Women’s Hospital
It really is the granular nature of what we do. It is knowing what it takes to get into the healthcare system and what these women are lacking in terms of support. It’s not just that we say, “you have to get to your appointment” but we take them to the appointment, we call them up and remind them that they have an appointment on Thursday, “the cab is gonna be there at 11”, and then if they don’t show up, we’re calling them to say, “what happened, is everything okay?”. No stone is left unturned. What we’re trying to say to the greater world is this is actually what health care is all about for those who lack resources. It has to be holistic. It has to be that you take into account the basics such as transportation, food, personal safety, housing, things like diapers, etc. And it’s because people who are experiencing poverty, hunger, homelessness, pregnancy, isolation, loneliness, lack of resources, language barriers – they need this level of support and resources because not having them does affect their health. Addressing the health of the mom during and after pregnancy affects the health of her baby. This is why the BTM Program is one that looks at the “whole health” of women.
(Rx): We live intersectional lives but our systems are very siloed. None of them are built to communicate with each other, let alone coordinate. From your perspective, what are some of those systemic policies or changes that you think need to be made so that more pregnant people facing a whole host of barriers can have healthy births and outcomes?
(Dr. Means): After all these years that I’ve been in medicine, it remains siloed. It’s also become incredibly more bureaucratic and administrative. When you have a patient that’s being discharged, it feels like it takes moving heaven and earth to get them from point A to point B. Providers are just not thinking about what happens before or after their visit. It’s not built for that. What happens to my patient when my patient leaves my department and goes outside the hospital walls? Where are they going to go?
We would like to think of Bridges to Moms as kind of a model that should be replicated for other populations. If you took 1,000 people with diabetes, for instance, and you wanted to get their blood sugar under control, it’s equally as important to know what percent of them are on food stamps, but the grocery store is over two miles away, and they don’t have money for public transportation as it is to know what medications to prescribe. You have to look at every single dimension, the social determinants. There’s no reason in the world why people can’t take that model and look at it for any population. “What about this particular patient who doesn’t speak English and doesn’t have a support system?” You really have to think about the different dimensions of that person’s life.
For instance, I can’t tell you the number of times we’ve gone to see a postpartum mom who has hypertension at their shelter. We bring in a little box of diapers, check their blood pressure and discover that it’s off the wall. Perhaps it’s because the obstetrician didn’t order the “meds to bed” – in other words, discharge the woman with a 90-day supply of medication. Instead, the prescription was sent to a pharmacy nearby the hospital, but the emergency shelter she was placed at ended up being 50 or 60 miles away. Without transportation, she can’t access the prescription. So the provider needs to know this fact to give the filled prescription to her before she leaves the hospital. If she has a hypertensive crisis and is 50 miles away, that woman may die.

Neonatologist, Dr. Silvia Patrizi (right), pictured with Dr. Roseanna Means (left) at Bridges to Moms’ Career Day event
PC: Brigham and Women’s Hospital
I visited a woman who was prescribed a blood pressure cuff to monitor her blood pressure. That’s great! But what happened was, she didn’t speak English so she couldn’t read the directions. The cuff also didn’t come with batteries. She only had batteries for her breast pump. She wasn’t feeling any symptoms from her blood pressure, so it didn’t feel as important to her, when compared to feeding her baby with the breast pump. Luckily for me, I brought my electronic blood pressure cuff when visiting her. I gave her my batteries for it. We explained in her native language the importance of taking her meds and checking her blood pressure every day. We connected her with primary care within a couple of weeks to check her again for her blood pressure, and I made sure that she had a ride to that appointment. The community health worker who spoke her language was with her for that appointment so she didn’t get lost. These are the kinds of things that everybody should be thinking about.
(Rx): What is your guiding North star?
(Dr. Means): I can’t say this without crying. I have many North Stars – my love for the women and incredible respect for what they’re going through and the warriors that they are.
Between my 1st and 2nd son, I had a baby girl that died at 27 weeks of pregnancy. We never really found out why she died. Of course, I had the home and the husband and the resources and the social worker that counseled me through my next pregnancy – I had all the support you could need. My baby’s name was Katharine. She was my little girl; I have three sons, it was my only little girl. When I started Bridges to Moms, the first case that they gave me was a woman who was 23-years-old. She had been targeted by a 48-year-old man when she was working at her part-time job at a fast food chain. They had a relationship and she got pregnant. She had no prenatal care and she ended up having a hypertensive crisis, which progressed to preeclampsia and was rushed to the Brigham. She had her baby girl, who weighed a pound and a half. The baby was at 27 weeks; and the mom’s name was Catherine. And so I thought, okay, that’s a message. This is what I’m supposed to do. This is the path. It was just really nice to see her baby get to her first birthday because she never ever would have survived without the help.
In our conversation, Dr. Means shared how BTM is working to expand their Workforce Development Training programs by welcoming new employers from various sectors like health care, childcare, and food services. If you are interested in learning more about or supporting BTM’s vital and life changing work visit the link below:
Job Opportunities
EqualHealth is a global community of health professionals, educators, and activists dedicated to achieving health justice through social medicine. For 13 years, we have trained health professionals to recognize the structural and social determinants of health and engage in thoughtful, coordinated activism that addresses the root causes of inequity. Our collaborative leadership and programming model centers leaders from Haiti, Uganda, and other Global South countries as the next generation of social medicine educators and practitioners.
Currently, they are hiring a part-time Development Lead to execute a highly effective funder strategy to support our critical work. Working between 12-15 hours each week, the Development Lead will collaborate with their activists and educators to elevate our funding infrastructure, securing sustainability through grant writing, donor support and a range of funding strategies. The development lead will be expected to study and understand the history, structure, objectives, and programs of EqualHealth to guide the development of funding strategies.
Empower Project is a nonprofit organization that works to get us back to the foundational roots of organizing. They have assisted groups with Relational Organizing in rural districts, urban and suburban districts, communities of color, and in multiple languages. Most importantly, they partner with progressive organizations and nonprofits, and work with leaders already engaged in targeted communities.
Currently, they are hiring a Data Manager and Analyst, who is highly independent, proactive, and self-motivated, and is skilled at prioritizing issues and digging into documentation and data. This position serves the dual role of assisting with technical and data support of client organizations using Empower, the industry-leading software for relational organizing, as well as providing data and automation support for Empower Project’s own internal organizing paid relational programs.
Events
Trust, Transparency, and Transformation: A conversation with funders | 3/28/24 at 2pm ET via Zoom
Join us on March 28, 2024 at 2pm Eastern for an hour-long moderated conversation that will bring together four panelists from Rx Foundation, The Healing Trust, CareQuest Institute for Oral Health, and Robert Wood Johnson Foundation to answer pre-submitted questions and speak authentically about their lessons learned, challenges, and how meaningful change happens in the funder landscape.

Recognizing that foundations often strive to be thoughtful and to embrace innovation and build trust, it’s also true that structures and approaches can challenge grantees- especially small mission-driven non-profits. The conversation aims to bridge that gap through elevating best practices, asking and answering the hard questions of “why” current practices exist and “why not” explore alternatives.
Recognizing that foundations often strive to be thoughtful and to embrace innovation and build trust, it’s also true that structures and approaches can challenge grantees- especially small mission-driven non-profits. The conversation aims to bridge that gap through elevating best practices, asking and answering the hard questions of “why” current practices exist and “why not” explore alternatives.
Participants are invited to anonymously submit questions about philosophy, process, practices, and improvements in advance. Moderator Jennifer Smith will both share an overview of themes and facilitate the discussion.
This session is presented as part of the Rx Foundation’s Power is a Social Determinant of Health series.

Connect With Us on Social Media
Follow-us on social media for the most up-to-date news, resources, and events from the Rx Foundation and its partners.